Domenico Di Ceglio set up the childhood and adolescent services at the Gender Identity Development Service (G.I.Ds) at the Tavistock. This is part two on a talk he gave at a conference on “Transgender” issues. You can find the rest of my series, on the Tavistock, below.
You can watch the talk on YouTube, below. 👇
Part one is here
This is the title of that talk. Transgender , Gender and Psychoanalysis, with this subtitle.

In part one Di Ceglie covers his motivation for setting up the children and adolescent service at G.I.Ds; the astronomic growth of referrals and the tensions between staff who wished to provide only therapeutic support, to children, and those who advocated for the administration of puberty blockers. As suggested by the title he uses metaphors to convey his role in managing these tensions. A psychoanalyst might suggest that this allows him to distance himself from the choices he made during his tenure.
We pick up at around the 30 minute mark. Di Ceglie is using the myth of Scylla and Charibdys, from Ulysses, to convey his position at the Tavistock. Both Scylla and Charibdys pose a risk to Ullyses and his sailors but only Charbdys can sink the ship. Ullysses, therefore, steers close to Scylla even though he knows she will snatch some of his sailors and crush them with her grip, before swallowing them. Di Ceglie clearly feels the service is under threat so he needs to balance these risks and sacrifices will have to be made.

Di Ceglie then reflects that it was the more valiant of Ulysses’ sailors who fell victim to Scylla and offers an explanation with reference to G.I.Ds staff calling them ”crusaders,” , which is very revealing.

He explains that the Tavistock tries to steer a middle way neither neglecting the mind nor the body. He claims that they work to break the cycle of secrecy and shame involved in an atypical gender identity. He further argues that the foster uncertainty about the outcomes for any child. I don’t see how this is compatible with this statement: If we are allowing a social transition and puberty blockers there is near certainty (98%) of progression to cross sex hormones. They will be sterile and, as we saw in part one, they will have near zero chance of any orgasmic capacity.

He is also keen to dispel any suggestion that they practice ”reparative” therapy i.e that they seek to reconcile the child with their sex/sexuality. I imagine this is motivated by the wish to avoid the fate of the Canadian Gender Clinic which he mentions more than once during the talk. (Ken Zucker’s clinic was accused of practicing conversion therapy on gender confused kids and his clinic shut down. He won a legal case but was not restored to his post)

He does share a case study of a natal male who adopted a female identity, following the death of his grandmother. After giving him some help to articulate his grief he reconciled to his sex and desisted.
He further claims that clinics who are rigid in their approach to these children run the risk of embedding the cross gender identity even further. He may be correct in this but, again, it does not square with the medical treatments. He does, thankfully, recognise an 80% desistance rate if allowed to go through a natural puberty; shame he does not include how many end up good old-fashioned homosexuals.
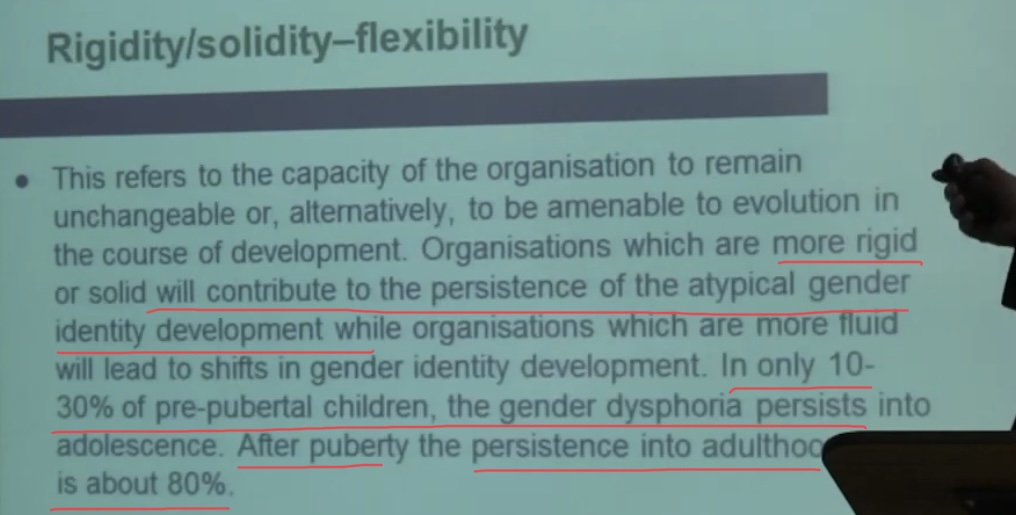
Clearly the clinic are making judgements that some children are unlikely to change their minds. This clip suggests early onset gender dysphoria is believed to be more intractable.
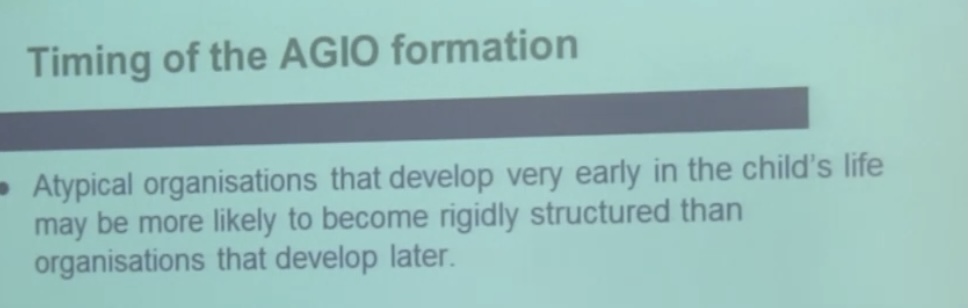
He next speculates that gender dysphoria is more intractable with those with paranoid schizophrenic tendencies and even those who have been subject to traumatic events in childhood. This is starting to echo the criteria used to dish out lobotomies or Electric Shock treatment.
Empathising versus Systematising.
This looks at the work of Simon Baron-Cohen who conducted research into children with atypical ”gender ” development and seems to be driven by defining certain behaviours more ”male” / “female” and, presumably, looking for evidence of “true trans“. Unsurprisingly females scored higher on empathy and men on systems. Between a likely biological predisposition and female socialisation women’s scores are , to me, unremarkable. What did surprise me was the scores for trans-identifying males. While they did score lower on “systemising”, than the control of males who were not identifying as ”transgender”, they also had lower scores for empathy. Curiously although Di Ceglie talks of the value of further research into identifying potential desisters this does not appear to have been a research area of interest to the staff at the Tavistock.
Di Ceglie claims it is possible to identify good candidates for early intervention. Not on e does he refer to detransitioners but they may not have been as significant a phenomenon when this conference took place. The YouTube video was uploaded two years ago but it may have pre-dated the Kiera Bell case. It would be interesting to know if he is paying attention to the rising rates of regret.
At the end of the conference Di Ceglie rushes through his final slides so I had to slow down the speed to take screen grabs. He has two slides on the benefits of early transition quoting research papers from 2006 i.e before the current surge in transgender kids /youth. He also claims that puberty blockers are ”considered to be fully reversible“ on one slide but look at the next slide, it directly contradicts this statement.
What are the risks?
It is unclear what the long term impact is on bone development, height, sex organ development it may affect brain development, and it may even lock in the Gender Dysphoria.
Those are some big risks!

Now we have a growing number of detransitioners the chickens may be comimg home to roost. Currently there are 35,000 members on the reddit detrans forum. It is growing at an alarming rate.
In part three I will cover the question and answer session.
You can support my work here. Every donation helps because we are up against billionaires funding this ideology, globally. Contrary to the propaganda I am not funded by Evangelical Christians, the Far Right or Viktor Orban. I rely on donations to cover my costs but do not donate if you are on a limited income.

Researching Gender Identity Ideology and it’s impact on our gay /autistic youth, kids in care as well as the sex based rights of women and adult homosexuals, especially Lesbians.
£10.00